The emergence of resistance to multiple antibiotics, pathogenic bacteria has become a major global public health threat. Resistant bacterial infections cause significant morbidity and mortality of patients and increase resistance to antibiotics poses a serious threat to antibiotics in the last 70 years for the great advances in medicine. Gained almost 95,000 people in 2005, for example, methicillin-resistant Staphylococcus aureus (MRSA) infections in the United States and 19,000 people died of MRSA infections – more than die from HIV / AIDS, emphysema, Parkinson’s disease and homicide combined. Without the development of innovative approaches to multi-drug resistant (MDR) pathogens fight, in many areas of medicine greatly affected, including surgery, prematurity care, cancer chemotherapy, care of critically ill patients and transplant medicine, all of which are only possible existence of effective antibiotic therapy. This complicates the increasing resistance of bacteria to antibiotics is currently approved by the lack of investment in the discovery of antibiotics in the pharmaceutical industry due to the inherently low yield of antibiotic in comparison with drugs/antibodies for chronic disease aligned. This situation is so bad that the World Health Organization MDR bacteria as one of the three greatest threats to human health identified and Infectious Diseases Society of America issued a call to action from the biomedical community to deal with the threat of MDR bacteria.
Although the development of new antibiotics is an approach to treat multidrug-resistant bacterial infections that only two new classes of antibiotics in the hospital were introduced in the last two decades, none of which are clearly still active against Gram-negative bacteria (Box 1). In addition, more bacteria develop resistance to any therapy based exclusively introduced to the bacteriostatic / bactericidal mechanism and clinically significant resistance, in a period of several months to years after the introduction of new antibiotics in the hospital. For example, daptomycin introduced into clinical practice in 2003 and less than a year later he observed the emergence of resistance in patients with Enterococcus faecium and MRSA infections. As a result, alternative approaches to combat bacterial infections urgently needed.
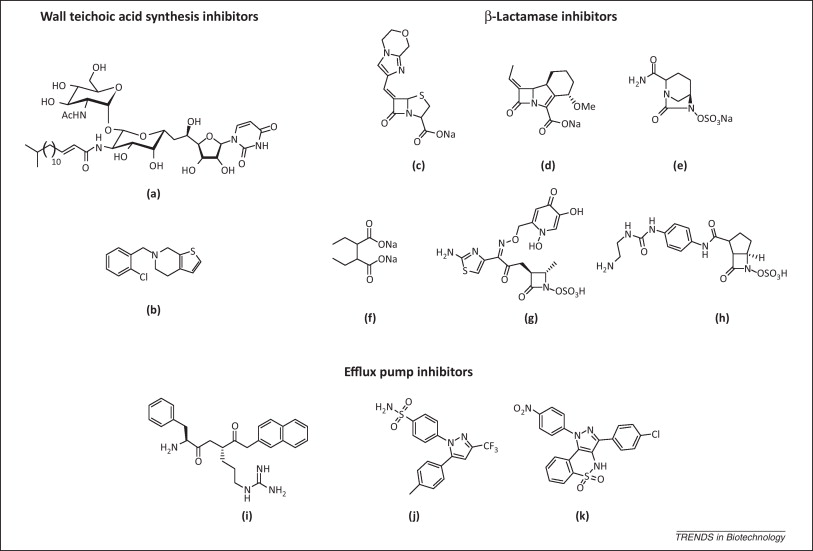
One such approach is to use a combination of drugs to combat MDR phenotype effect. Such efforts are antibiotics and antibiotic combinations clutch antibiotic adjuvant molecules directly nonantibiotic mechanisms of resistance objectives such as the inhibition of β-lactamase enzyme or indirectly influencing the bacterial resistance of the target paths as FCS. Screening of libraries already approved drugs as a means for the identification of non-trivial antimicrobial adjuvant was also tested. The aim of this review is to provide the reader with an overview of the approach and highlights the recent progress in each area. It is not designed to fight a comprehensive review of approaches to antibiotic resistance, which would be beyond the scope of this document.